Background: Closed-loop ventilators (CLVs): CLVs also known as automated ventilators, are advanced systems that automatically adjust ventilator settings based on the patient’s respiratory mechanics. Unlike open-loop ventilators (OLVs), which require manual parameter adjustments, CLVs use real-time feedback to maintain target oxygen saturation (SpO2) and end-tidal carbon dioxide (EtCO2) levels, enhancing patient comfort and reducing complications. Cerebral Protection in Traumatic Brain Injury (TBI): Maintaining normoxia, and normocapnia is crucial for cerebral protection in TBI. High carbon dioxide (CO2) levels cause vasodilation, increasing intracranial pressure, while low levels cause vasoconstriction, reducing cerebral perfusion. CLVs automatically adjust ventilator settings based on continuous patient feedback, optimizing CO2 levels and cerebral blood flow (CBF). Case Presentation: A 19-year-old male with severe TBI was intubated and connected to a fully automated CLV and set to "Brain Injury" mode. The ventilator automatically adjusted parameters to achieve target end-tidal carbon dioxide (EtCO2) levels, evidenced by subsequent arterial blood gas (ABG) results showing desired partial pressure of carbon dioxide (pCO2) and partial pressure of oxygen (pO2) levels. Conclusion: CLVs in TBI patients automatically manage CO2 elimination and oxygen delivery using simplified settings, adjusting based on real-time oxygen saturation (SpO2) and EtCO2 levels. This approach maintains normocapnia and normoxia, meeting cerebral protection criteria with fewer manual adjustments, advantageous in the emergency department (ED). CLVs offer a practical solution in the ED, automating ventilator adjustments to maintain desired CO2 levels, thus shifting the clinician's role from manual “presetting” to “deciding” target CO2 levels. This automation improves efficiency and patient outcomes in a hectic clinical environment.
| Published in | Frontiers (Volume 4, Issue 4) |
| DOI | 10.11648/j.frontiers.20240404.15 |
| Page(s) | 150-155 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Closed-Loop Ventilation, Adaptive Support Ventilation, Artificial Intelligence, Cerebral Protection, Traumatic Brain Injury
Time | EtCO2 Level (mmHg) | pCO2 Level (mmHg) |
|---|---|---|
1st Hour | 35 | 38.4 |
2nd Hour | 35 | 36.2 |
3rd Hour | 38 | 37.7 |
4th Hour | 36 | 40.3 |
CLV | Closed-Loop Ventilation |
OLV | Open-Loop Ventilation |
SpO2 | Oxygen Saturation |
EtCO2 | End-tidal Carbon Dioxide |
TBI | Traumatic Brain Injury |
CO2 | Carbon Dioxide |
CBF | Cerebral Blood Flow |
ABG | Arterial Blood Gas |
pCO2 | Partial Pressure of Carbon Dioxide |
pO2 | Partial Pressure of Oxygen |
ED | Emergency Department |
VILI | Ventilator-induced Lung Injury |
AI | Artificial Intelligence |
ASV | Adaptive Support Ventilator |
CT | Computerized Tomography |
ARDS | Acute Respiratory Distress Syndrome |
PEEP | Positive End Expiratory Pressure |
FiO2 | Fractionated of Inspired Oxygen |
%MinVol | Percentage of Minute Volume |
O2 | Oxygen |
Vt | Tidal Volume |
f | Respiratory Rate |
Psupp | Pressure Support |
I: E Ratio | Inspiratory: Expiratory Ratio |
| [1] |
Arora S, Singh PM, Trikha A. Ventilatory strategies in trauma patients. J Emerg Trauma Shock. 2014; 7(1): 25-31.
https://doi.org/10.4103/0974-2700.125635 (Frontiers). |
| [2] | Miller JD, Ledingham IM. Reduction of increased intracranial pressure: Comparison between hyperbaric oxygen and hyperventilation. Arch Neurol. 1971; 24(3): 210-6. |
| [3] |
Botta M, Wenstedt EFE, Tsonas AM, Buiteman-Kruizinga LA, van Meenen DMP, Korsten HHM, et al. Effectiveness, safety, and efficacy of INTELLiVENT–adaptive support ventilation, a closed-loop ventilation mode for use in ICU patients: a systematic review. Expert Review of Respiratory Medicine. 2021; 15(11): 1403-13.
https://doi.org/10.1080/17476348.2021.1990008 (SpringerLink). |
| [4] | Anan'ev EP, Polupan AA, Matskovskiy IV, Oshorov AV, Goryachev AS, Savin IA, et al. Use of the IntelliVent-ASV mode for maintaining the target EtCO2 range in patients with severe TBI. Zh Vopr Neirokhir Im NN Burdenko. 2017; 81(5): 63-8. |
| [5] | Arnal JM, Garnero A, Novotni D, Corno G, Donati SY, Demory D, Quintana G, Ducros L, Laubscher T, Durand-Gasselin J. Closed-loop ventilation mode for critically ill patients: A prospective clinical study. Minerva Anestesiologica. 2018; 84(1): 58-67. Available from: |
| [6] | Borsellino B, Schultz MJ, Gama de Abreu M, Robba C, Bilotta F. Mechanical ventilation in neurocritical care patients: a systematic literature review. Expert Review of Respiratory Medicine.2016; 10(10): 1123-1132. |
| [7] | Lellouche F, Bouchard P-A, L’Her E. Automated ventilation tailored to the patient’s needs: Clinical potential and technological development. Critical Care. 2017; 21(1): 240. |
| [8] | Bialais E, Wittebole X, Vignaux L, Roeseler J, Wysocki M, Meyer J, Reychler G, Novotni D, Sottiaux T, Laterre PF, Hantson P. Closed-loop ventilation mode in intensive care: A prospective clinical study. Minerva Anestesiologica. 2016; 82(6): 657-68. Available from: |
| [9] | Wendel Garcia PD, Hofmaenner DA, Brugger SD, Acevedo CT, Bartussek J, Camen G, Bader PR, Bruellmann G, Kattner J, Ganter C, Schuepbach RA, Buehler PK. Closed-loop ventilation versus conventional ventilation in ICU patients: A prospective study. Journal of Intensive Care Medicine. 2021; 36(10): 1184-1193.. Available from: |
| [10] | Arnal JM, Saoli M, Garnero A. Ventilatory management in ICU patients: A clinical overview. Heart & Lung. 2020; 49(4): 427-434. Available from: |
| [11] | Chelly J, Mazerand S, Jochmans S, Weyer CM, Pourcine F, Ellrodt O, Thieulot-Rolin N, Serbource-Goguel J, Sy O, Vong LVP, Monchi M. Impact of a closed-loop ventilation mode on ICU patient outcomes: A prospective study. Critical Care. 2020; 24(1): 453. Available from: |
| [12] | Abutbul A, Sviri S, Zbedat W, Linton DM, van Heerden PV. Evaluation of ventilatory support in critically ill patients using a novel approach. South African Journal of Critical Care. 2014; 30(1): 28-32. |
| [13] | Beijers AJ, Roos AN, Bindels AJ. A case report on the management of acute respiratory distress using advanced ventilatory support. Intensive Care Medicine. 2014; 40(5): 752-3. Available from: |
| [14] | Sulemanji DS, Marchese A, Wysocki M, Kacmarek RM. A comparative study of ventilation strategies in critically ill patients. Intensive Care Medicine. 2013; 39(4): 703-10.. Available from: |
| [15] | Brower RG, Lanken PN, MacIntyre N, Matthay MA, Morris A, Ancukiewicz M, Schoenfeld D, Thompson BT; National Heart, Lung, and Blood Institute ARDS Clinical Trials Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. New England Journal of Medicine. 2004; 351(4): 327-36. Available from: |
APA Style
Azmi, F. I. M., Shah, N. F. A. F., Azhar, A. M. N. (2024). Enhancing Cerebral Protection: A Closed-Loop Ventilation Approach (Artificial Intelligence) for Targeted Carbon Dioxide Regulation in Traumatic Brain Injury. Frontiers, 4(4), 150-155. https://doi.org/10.11648/j.frontiers.20240404.15
ACS Style
Azmi, F. I. M.; Shah, N. F. A. F.; Azhar, A. M. N. Enhancing Cerebral Protection: A Closed-Loop Ventilation Approach (Artificial Intelligence) for Targeted Carbon Dioxide Regulation in Traumatic Brain Injury. Frontiers. 2024, 4(4), 150-155. doi: 10.11648/j.frontiers.20240404.15
AMA Style
Azmi FIM, Shah NFAF, Azhar AMN. Enhancing Cerebral Protection: A Closed-Loop Ventilation Approach (Artificial Intelligence) for Targeted Carbon Dioxide Regulation in Traumatic Brain Injury. Frontiers. 2024;4(4):150-155. doi: 10.11648/j.frontiers.20240404.15
@article{10.11648/j.frontiers.20240404.15,
author = {Fatin Izzati Mohammed Azmi and Nur Fazliatul Azrin Farouk Shah and Abdul Muhaimin Noor Azhar},
title = {Enhancing Cerebral Protection: A Closed-Loop Ventilation Approach (Artificial Intelligence) for Targeted Carbon Dioxide Regulation in Traumatic Brain Injury
},
journal = {Frontiers},
volume = {4},
number = {4},
pages = {150-155},
doi = {10.11648/j.frontiers.20240404.15},
url = {https://doi.org/10.11648/j.frontiers.20240404.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.frontiers.20240404.15},
abstract = {Background: Closed-loop ventilators (CLVs): CLVs also known as automated ventilators, are advanced systems that automatically adjust ventilator settings based on the patient’s respiratory mechanics. Unlike open-loop ventilators (OLVs), which require manual parameter adjustments, CLVs use real-time feedback to maintain target oxygen saturation (SpO2) and end-tidal carbon dioxide (EtCO2) levels, enhancing patient comfort and reducing complications. Cerebral Protection in Traumatic Brain Injury (TBI): Maintaining normoxia, and normocapnia is crucial for cerebral protection in TBI. High carbon dioxide (CO2) levels cause vasodilation, increasing intracranial pressure, while low levels cause vasoconstriction, reducing cerebral perfusion. CLVs automatically adjust ventilator settings based on continuous patient feedback, optimizing CO2 levels and cerebral blood flow (CBF). Case Presentation: A 19-year-old male with severe TBI was intubated and connected to a fully automated CLV and set to "Brain Injury" mode. The ventilator automatically adjusted parameters to achieve target end-tidal carbon dioxide (EtCO2) levels, evidenced by subsequent arterial blood gas (ABG) results showing desired partial pressure of carbon dioxide (pCO2) and partial pressure of oxygen (pO2) levels. Conclusion: CLVs in TBI patients automatically manage CO2 elimination and oxygen delivery using simplified settings, adjusting based on real-time oxygen saturation (SpO2) and EtCO2 levels. This approach maintains normocapnia and normoxia, meeting cerebral protection criteria with fewer manual adjustments, advantageous in the emergency department (ED). CLVs offer a practical solution in the ED, automating ventilator adjustments to maintain desired CO2 levels, thus shifting the clinician's role from manual “presetting” to “deciding” target CO2 levels. This automation improves efficiency and patient outcomes in a hectic clinical environment.
},
year = {2024}
}
TY - JOUR T1 - Enhancing Cerebral Protection: A Closed-Loop Ventilation Approach (Artificial Intelligence) for Targeted Carbon Dioxide Regulation in Traumatic Brain Injury AU - Fatin Izzati Mohammed Azmi AU - Nur Fazliatul Azrin Farouk Shah AU - Abdul Muhaimin Noor Azhar Y1 - 2024/12/30 PY - 2024 N1 - https://doi.org/10.11648/j.frontiers.20240404.15 DO - 10.11648/j.frontiers.20240404.15 T2 - Frontiers JF - Frontiers JO - Frontiers SP - 150 EP - 155 PB - Science Publishing Group SN - 2994-7197 UR - https://doi.org/10.11648/j.frontiers.20240404.15 AB - Background: Closed-loop ventilators (CLVs): CLVs also known as automated ventilators, are advanced systems that automatically adjust ventilator settings based on the patient’s respiratory mechanics. Unlike open-loop ventilators (OLVs), which require manual parameter adjustments, CLVs use real-time feedback to maintain target oxygen saturation (SpO2) and end-tidal carbon dioxide (EtCO2) levels, enhancing patient comfort and reducing complications. Cerebral Protection in Traumatic Brain Injury (TBI): Maintaining normoxia, and normocapnia is crucial for cerebral protection in TBI. High carbon dioxide (CO2) levels cause vasodilation, increasing intracranial pressure, while low levels cause vasoconstriction, reducing cerebral perfusion. CLVs automatically adjust ventilator settings based on continuous patient feedback, optimizing CO2 levels and cerebral blood flow (CBF). Case Presentation: A 19-year-old male with severe TBI was intubated and connected to a fully automated CLV and set to "Brain Injury" mode. The ventilator automatically adjusted parameters to achieve target end-tidal carbon dioxide (EtCO2) levels, evidenced by subsequent arterial blood gas (ABG) results showing desired partial pressure of carbon dioxide (pCO2) and partial pressure of oxygen (pO2) levels. Conclusion: CLVs in TBI patients automatically manage CO2 elimination and oxygen delivery using simplified settings, adjusting based on real-time oxygen saturation (SpO2) and EtCO2 levels. This approach maintains normocapnia and normoxia, meeting cerebral protection criteria with fewer manual adjustments, advantageous in the emergency department (ED). CLVs offer a practical solution in the ED, automating ventilator adjustments to maintain desired CO2 levels, thus shifting the clinician's role from manual “presetting” to “deciding” target CO2 levels. This automation improves efficiency and patient outcomes in a hectic clinical environment. VL - 4 IS - 4 ER -
Department of Emergency Medicine, University Malaya Medical Centre, Kuala Lumpur, Malaysia
Biography: Fatin Izzati Mohammed Azmi is a medical officer and postgraduate resident at the University Malaya Medical Centre, Emergency Medicine Department. She completed her Bachelor’s in Medicine and Bachelor’s in Surgery (MBBS) in MSU-International Medical School, Bangalore, India in 2013. She is now undergoing her Master’s Degree in Emergency Medine in University Malaya, Malaysia. She completed her housemenship training for 2 years in Hospital Sultanah Nur Zahirah, Kuala Terengganu, Malaysia and pursued her placement as medical officer in Emergency Department in the same hospital before pursuing her Master’s programme in current hospital.

Department of Emergency Medicine, University Malaya Medical Centre, Kuala Lumpur, Malaysia
Department of Emergency Medicine, University Malaya Medical Centre, Kuala Lumpur, Malaysia

Figure 1. CT Brain showing intracranial haemorrhage.
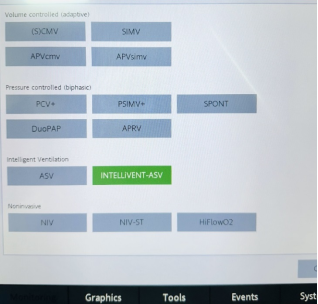
Figure 2. Option for ASV mode.
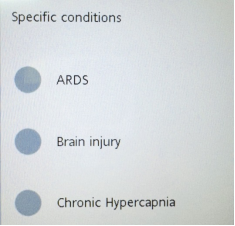
Figure 3. Options available for ARDS, Chronic Hypercapnia and Brain Injury.
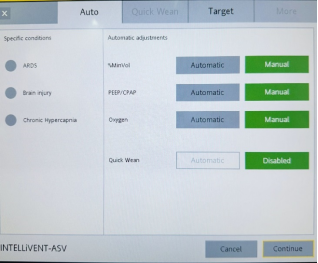
Figure 4. Options for automatic adjustments.
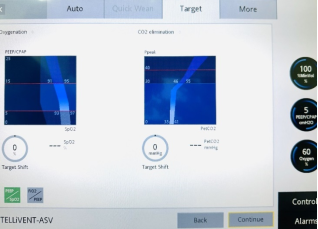
Figure 5. Options for target SpO2 and EtCO2 ranges.
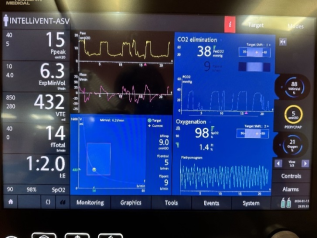
Figure 6. Visual interface of ventilator using ASV mode displaying CO2 elimination and Oxygenation with real-time EtCO2 and SpO2 within target range.

